This pathway covers management of pressure ulcers/injuries (PUs/PIs).
Decision Nodes
Patient and PU/PI assessment
1) History of Present Illness
2) Physical Exam
3) Risk Assessment- Braden Scale
4) Nutritional Screening and Assessment
5) Equipment and Seating Evaluations
Q: Setting in which patient developed PU/PI (inpatient, outpatient, etc)?
Q: Location of ulcer?
Q: Age, gender
Q: Onset of ulcer?
Q: Pain?
Q: History of previous PU/PI?
Q: Prior Treatment/Prevention: Previous employment of pressure relieving and redistributing maneuvers/devices;Past surgical history related to PU/PI and complications
Q: Medications
Q: Social History
Q: Physical Exam notes/findings:
Q: Ulcer/Injury Exam notes/findings:
Q: Type of scale/test used and result:
Q: Nutritional Assessment notes/findings:
Q: Functional, Equipment, and Seating Evaluation notes/findings:
Determine PU/PI Classification/Staging
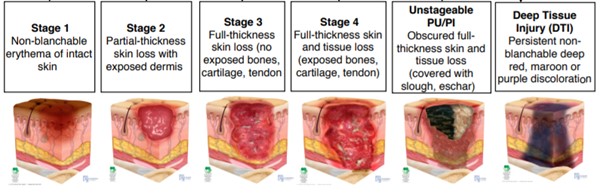
PU/PI Stages drawings by NPUAP copyright & used with permission
Q: Which staging is most consistent with assessment? Stage 1;Stage 2;Stage 3;Stage 4 ;Unstageable PU/PI ;Deep Tissue Injury (DTI)
Is the ulcer located on the lower extremities?
Determine if healable, maintenance or non-healable
- Healable wound: the cause is corrected, there is enough blood supply to heal;
moist interactive healing
- Maintenance wound: the wound could heal, but the cause is not corrected
due to patient unwillingness to adhere to treatment or a lack of required system
resources
- Non-healable wound: the patient is ill or may have negative protein balance or
inadequate blood supply that is not bypassable or dilatable
Q: Is the ulcer healable? Healable ;Non-healable;Maintenance
Conduct noninvasive arterial tests
Q: ABI results? Normal (values) ;Abnormal (values)
Is hospital admission indicated?
If any of the following are selected -> yes
If none are selected -> no
Q: Does the patient show signs of any of the following? Surgical debridement needed (e.g. extensive necrosis) ;Postoperatice complications requiring surgical interventon;Systemic infection (e.g. sepsis or SIRS) ;Necrotizing soft tissue infection
Manage according to Staging
STAGE 1: Manage underlying causes
STAGE 2: Manage underlying causes
Q: Interventions for management of underlying causes
STAGE 3: Manage underlying causes
- Pressure redistribution: if large or multiple stage 3 or 4 ulcers on trunk or pelvis, or if patient has recently had a flap to close PU/PI, may use group 2 support surfaces (powered air flotation beds, powered pressure reducing air mattresses, non-powered advanced pressure reducing mattresses). If PU/PI is on heel: completely offload the heel
- Reposition patient and encourage mobility, if not contraindicated
- Optimize nutrition
- Address excessive moisture and shear: manage incontinence if needed
Q: Interventions for management of underlying causes
STAGE 4: Manage underlying causes
- Pressure redistribution:
- if large or multiple stage 3 or 4 ulcers on trunk or pelvis, or if patient has recently had a flap to close PU/PI, may use group 2 support surfaces (powered air flotation beds, powered pressure reducing air mattresses, non-powered advanced pressure reducing mattresses). If PU/PI is on heel: completely offload the heel. Sitting on wheelchair is not recommended except for emergencies or important issues.
- Reposition patient and encourage mobility, if not contraindicated
- Optimize nutrition
- Address excessive moisture and shear: manage incontinence if needed
Q: Interventions for management of underlying causes
UNSTAGEABLE: Manage underlying causes
Q: Interventions for management of underlying causes
DTI: Manage underlying causes
Local Wound Care for Stage 1
Q: Notes
Local Wound Care for Stage 2
Comprehensive local wound care including cleansing, control of bioburden, barrier cream or wound moisture balance with appropriate dressing and periwound skin protection
| Healable | Non-healable/maintenance |
| Cleansing | - Gently cleanse with sterile saline, water, 0.5-1% acetic acid, or wound cleanser
- If solution cannot be retrieved/aspirated (due to undermining, sinuses, etc.), use forceps to hold moistened gauze ribbons and cleanse the wound. Ensure all gauze is retrieved.
| - Keep wound bed dry
- May cleanse ulcers with antiseptic agents to help manage bioburden, odor and moisture
|
| Debridement | - Stage 1 and 2 PU/PI: debridement not indicated
| - For Stage 1 and 2: do not debride
|
| Infection and Bioburden Control | - If no signs of infection, do not use antimicrobial dressings
- If clinical signs of local infection or no healing is seen within 2 weeks of debridement and pressure redistribution, collect wound culture post debridement and initiate topical antimicrobials
- If spreading or systemic infection, collect wound culture post debridement and initiate systemic antibiotics and topical antimicrobials
- Antimicrobial dressings (with PHMB, cadexomer iodine, silver sulfadiazine, other silver products, honey):
| - If clinical signs of local infection, collect wound culture post debridement or gentle removal of necrotic tissue and initiate topical antimicrobials
- If spreading or systemic infection, collect wound culture post debridement or gentle removal of necrotic tissue and initiate systemic antibiotics and topical antimicrobials
- Topic antimicrobials:
- If minimal/ light exudate, consider painting wound with antiseptic solution or using a topical antimicrobial agent
- If moderate or heavy exudate, consider non-adherent antimicrobial dressings (with silver, cadexomer iodine, medical-grade honey, silver, etc):
|
| Peri-wound skin care | - If excessive exudate: use zinc, dimethicone, silicone-based skin protectant, or skin prep to protect periwound
- If dry skin use moisturizer with humectants for skin hydration
| - If excessive exudate: use zinc, dimethicone, silicone-based skin protectant, or skin prep to protect periwound
- If dry skin use moisturizer with humectants for skin hydration
|
| Moisture Balance | - Dressing choice depends on ulcer characteristics, clinical experience, patient preference, care setting and cost.
- Maintain wound moisture or provide moisture to dry wounds with:
- Manage exudate with:
| - Keep wound dry.
- If exudate: apply appropriate non-adherent dressing
- Avoid conventional dressing products that require daily dressing changes.
|
Q: Ulcer/injury treated as healable or non-healable? Healable;Non-healable
Q: Local wound care notes
Q: Notes
Local Wound Care for Stage 3
- Comprehensive local wound care including cleansing, debridement, control of bioburden, wound moisture balance with appropriate dressings and periwound skin protection
| Healable | Non-healable/maintenance |
| Cleansing | - Gently cleanse with sterile saline, water, 0.5-1% acetic acid, or wound cleanser
- If solution cannot be retrieved/aspirated (due to undermining, sinuses, etc.), use forceps to hold moistened gauze ribbons and cleanse the wound. Ensure all gauze is retrieved.
| - Keep wound bed dry
- May cleanse ulcers with antiseptic agents to help manage bioburden, odor and moisture
|
| Debridement | - Stages 3 and 4 PU/PI, unstageable PU/PI due to slough/eschar: debridement indicated for removal of devitalized tissue at initial assessment and on a regular basis until wound bed is covered with granulation tissue; for wounds with no signs of improvement despite standard care for 2 - 4 weeks; and for infected wounds.
- If dry eschar in ischemic limb: do not debride; monitor for signs of infection
- Choice of debridement methods:
- Choice depends on patient condition and resources (clinician's skills, license restrictions, resources available).
- For PU/PI with extensive necrosis, Stage 3 or 4 with undermining, sinus tracts or signs of infection (i.e. advancing cellulitis, crepitus, fluctuance, and/or sepsis secondary to ulcer-related infection): initial surgical debridement in the operating room is recommended
- If there is no urgent clinical need for drainage or removal of devitalized tissue: sharp conservative, mechanical, enzymatic, autolytic and/or biological debridement may be used
- Sensate patients may not tolerate sharp debridement at the bed side and may need to be debrided in the operating room
| - For dry, stable eschars without fluctuance or erythema: do not debride
- For Stage 3 and 4 PUs/PIs: conservative debridement of nonviable tissue only
- For PU/PI with extensive necrosis or signs of infection (i.e. advancing cellulitis, crepitus, fluctuance, and/or sepsis secondary to ulcer-related infection): initial surgical debridement in the operating room may be considered if this intervention is aligned with the patient's and caregiver's goals
|
| Infection and Bioburden Control | - If no signs of infection, do not use antimicrobial dressings
- If clinical signs of local infection or no healing is seen within 2 weeks of debridement and pressure redistribution, collect wound culture post debridement and initiate topical antimicrobials
- If spreading or systemic infection, collect wound culture post debridement and initiate systemic antibiotics and topical antimicrobials
- Antimicrobial dressings (with PHMB, cadexomer iodine, silver sulfadiazine, other silver products, honey):
- Osteomyelitis should be considered if ulcer probes to bone
| - If clinical signs of local infection, collect wound culture post debridement or gentle removal of necrotic tissue and initiate topical antimicrobials
- If spreading or systemic infection, collect wound culture post debridement or gentle removal of necrotic tissue and initiate systemic antibiotics and topical antimicrobials
- Topic antimicrobials:
- If minimal/ light exudate, consider painting wound with antiseptic solution or using a topical antimicrobial agent
- If moderate or heavy exudate, consider non-adherent antimicrobial dressings (with silver, cadexomer iodine, medical-grade honey, silver, etc):
- Osteomyelitis should be considered if ulcer probes to bone
|
| Peri-wound skin care | - If excessive exudate: use zinc, dimethicone, silicone-based skin protectant, or skin prep to protect periwound
- If dry skin use moisturizer with humectants for skin hydration
| - If excessive exudate: use zinc, dimethicone, silicone-based skin protectant, or skin prep to protect periwound
- If dry skin use moisturizer with humectants for skin hydration
|
| Moisture Balance | - Dressing choice depends on ulcer characteristics, clinical experience, patient preference, care setting and cost.
- Maintain wound moisture or provide moisture to dry wounds with:
- Manage exudate with:
- Fill deep wounds to avoid dead space. Do not pack wounds tightly
| - Keep wound dry.
- If exudate: apply appropriate non-adherent dressing
- Fill deep wounds to avoid dead space. Do not pack wounds tightly
- Avoid conventional dressing products that require daily dressing changes.
|
Q: Pressure ulcer/injury treated as healable or non-healable? Healable;Non-healable
Q: Local wound care notes
Q: Notes
Local Wound Care for Stage 4
- Comprehensive local wound care including cleansing, debridement, control of bioburden, wound moisture balance with appropriate dressings and periwound skin protection
- If ulcer probes to the bone, evaluate for osteomyelitis
| Healable | Non-healable/maintenance |
| Cleansing | - Gently cleanse with sterile saline, water, 0.5-1% acetic acid, or wound cleanser
- If solution cannot be retrieved/aspirated (due to undermining, sinuses, etc.), use forceps to hold moistened gauze ribbons and cleanse the wound. Ensure all gauze is retrieved.
| - Keep wound bed dry
- May cleanse ulcers with antiseptic agents to help manage bioburden, odor and moisture
|
| Debridement | - Stages 3 and 4 PU/PI, unstageable PU/PI due to slough/eschar: debridement indicated for removal of devitalized tissue at initial assessment and on a regular basis until wound bed is covered with granulation tissue; for wounds with no signs of improvement despite standard care for 2 - 4 weeks; and for infected wounds.
- If dry eschar in ischemic limb: do not debride; monitor for signs of infection
- Choice of debridement methods:
- Choice depends on patient condition and resources (clinician's skills, license restrictions, resources available).
- For PU/PI with extensive necrosis, Stage 3 or 4 with undermining, sinus tracts or signs of infection (i.e. advancing cellulitis, crepitus, fluctuance, and/or sepsis secondary to ulcer-related infection): initial surgical debridement in the operating room is recommended
- If there is no urgent clinical need for drainage or removal of devitalized tissue: sharp conservative, mechanical, enzymatic, autolytic and/or biological debridement may be used
- Sensate patients may not tolerate sharp debridement at the bed side and may need to be debrided in the operating room
| - For dry, stable eschars without fluctuance or erythema: do not debride
- For Stage 3 and 4 PUs/PIs: conservative debridement of nonviable tissue only
- For PU/PI with extensive necrosis or signs of infection (i.e. advancing cellulitis, crepitus, fluctuance, and/or sepsis secondary to ulcer-related infection): initial surgical debridement in the operating room may be considered if this intervention is aligned with the patient's and caregiver's goals
|
| Infection and Bioburden Control | - If no signs of infection, do not use antimicrobial dressings
- If clinical signs of local infection or no healing is seen within 2 weeks of debridement and pressure redistribution, collect wound culture post debridement and initiate topical antimicrobials
- If spreading or systemic infection, collect wound culture post debridement and initiate systemic antibiotics and topical antimicrobials
- Antimicrobial dressings (with PHMB, cadexomer iodine, silver sulfadiazine, other silver products, honey):
- Osteomyelitis should be considered if ulcer probes to bone
| - If clinical signs of local infection, collect wound culture post debridement or gentle removal of necrotic tissue and initiate topical antimicrobials
- If spreading or systemic infection, collect wound culture post debridement or gentle removal of necrotic tissue and initiate systemic antibiotics and topical antimicrobials
- Topic antimicrobials:
- If minimal/ light exudate, consider painting wound with antiseptic solution or using a topical antimicrobial agent
- If moderate or heavy exudate, consider non-adherent antimicrobial dressings (with silver, cadexomer iodine, medical-grade honey, silver, etc):
- Osteomyelitis should be considered if ulcer probes to bone
|
| Peri-wound skin care | - If excessive exudate: use zinc, dimethicone, silicone-based skin protectant, or skin prep to protect periwound
- If dry skin use moisturizer with humectants for skin hydration
| - If excessive exudate: use zinc, dimethicone, silicone-based skin protectant, or skin prep to protect periwound
- If dry skin use moisturizer with humectants for skin hydration
|
| Moisture Balance | - Dressing choice depends on ulcer characteristics, clinical experience, patient preference, care setting and cost.
- Maintain wound moisture or provide moisture to dry wounds with:
- Manage exudate with:
- Fill deep wounds to avoid dead space. Do not pack wounds tightly
| - Keep wound dry.
- If exudate: apply appropriate non-adherent dressing
- Fill deep wounds to avoid dead space. Do not pack wounds tightly
- Avoid conventional dressing products that require daily dressing changes.
|
Q: Pressure ulcer/injury treated as healable or non-healable? Healable;Non-healable
Q: Local wound care notes
Q: Notes
Local Wound Care for Unstageable PU/PI
Conduct debridement: stage can only be determined when enough slough and/or eschar is removed to expose the anatomic depth of soft tissue damage involved
| Healable | Non-healable/maintenance |
| Cleansing | - Gently cleanse with sterile saline, water, 0.5-1% acetic acid, or wound cleanser
- If solution cannot be retrieved/aspirated (due to undermining, sinuses, etc.), use forceps to hold moistened gauze ribbons and cleanse the wound. Ensure all gauze is retrieved.
| - Keep wound bed dry
- May cleanse ulcers with antiseptic agents to help manage bioburden, odor and moisture
|
| Debridement | - Stages 3 and 4 PU/PI, unstageable PU/PI due to slough/eschar: debridement indicated for removal of devitalized tissue at initial assessment and on a regular basis until wound bed is covered with granulation tissue; for wounds with no signs of improvement despite standard care for 2 - 4 weeks; and for infected wounds.
- If dry eschar in ischemic limb: do not debride; monitor for signs of infection
- Choice of debridement methods:
- Choice depends on patient condition and resources (clinician's skills, license restrictions, resources available).
- For PU/PI with extensive necrosis, Stage 3 or 4 with undermining, sinus tracts or signs of infection (i.e. advancing cellulitis, crepitus, fluctuance, and/or sepsis secondary to ulcer-related infection): initial surgical debridement in the operating room is recommended
- If there is no urgent clinical need for drainage or removal of devitalized tissue: sharp conservative, mechanical, enzymatic, autolytic and/or biological debridement may be used
- Sensate patients may not tolerate sharp debridement at the bed side and may need to be debrided in the operating room
| - For dry, stable eschars without fluctuance or erythema: do not debride
- For Stage 3 and 4 PUs/PIs: conservative debridement of nonviable tissue only
- For PU/PI with extensive necrosis or signs of infection (i.e. advancing cellulitis, crepitus, fluctuance, and/or sepsis secondary to ulcer-related infection): initial surgical debridement in the operating room may be considered if this intervention is aligned with the patient's and caregiver's goals
|
Q: Notes
Local Wound Care for DTI
- Protect affected skin with moisture barrier products and skin protectants
- DTI can quickly evolve to Stage 3 or 4 PU/PI despite adequate care. If this evolvement occurs, PU/PI should be managed as Stage 3 or 4 accordingly
- There are anecdotal data on the use of non-contact low frequency ultrasound for deep tissue injury [12][13]
Q: Notes
For healable ulcers: signs of improvement in 2-4 weeks?
Q: Notes
Continue treatment until completed healing, prevent new PU/PI
Q: For all healable PUs/PIs: Check differential diagnoses
Q: For all healable PUs/PIs: is the cause being adequately addressed? Checked for adequate pressure redistribution, repositioning, transfer and plan to increase mobility;Checked for adequate glycemic control and nutritional intake;Checked for adequate moisture/incontinence management;Checked for any co-factors that may be impeding healing (e.g., medications, smoking, immunosuppression, etc).;Checked for soft tissue infection and/or osteomyelitis;If applicable: checked for presence of any "acquired bursa" between the skin and underlying bone or at the base of the ulcer.;If ulcer is on lower extremity: checked for adequate vascular supply to the ulcer
Q: For all healable PUs/PIs: are patient's concerns addressed?
Q: For all healable PUs/PIs: is local wound care adequate? Debridement: checked for adequate removal of devitalized tissue and surrounding callus;Bioburden: checked for adequate management;Dressings: checked for excess exudate management, periwound protection, moist wound bed
Q: For infected PUs/PIs: assess the following factors Checked for presence of unidentified necrotic soft tissue or bone;Checked for presence of an undrained abscess;Checked for presence of osteomyelitis that has not yet responded;Checked for presence of an untreated or an unidentified pathogen;Checked for presence of an antibiotic delivery problem;Checked for presence of an antibiotic non adherence issue;Checked for correction of any metabolic aberrations
Create new care plan
- Generate care plan that addresses any factors or co-morbidities impairing healing
- Biopsy or swab with validated method such as Levine technique to rule out infection/ osteomyelitis.
- Consider use of adjunctive therapy
- For large ulcers, if important anatomical structures are exposed (e.g., vessels, tendon, nerves), or if osteomyelitis is present, consider surgical reconstruction with flaps if ulcer is large
- Place consults/referrals as needed: Infectious disease specialist, physical therapist, occupational therapist, plastic surgeon, vascular specialist, behavioral medicine
- Create task to follow up: click here